
|

 One of the strongest and most far-reaching current trends in health care is the application of evidence - based practice through the development of research and information technology/informatics. This trend is visible across all sectors of nursing, including practice, education, research, and administration. The rationale behind this trend is to improve client care by selecting best practice options grounded in viable research, and to expand the theoretical foundations of all health professions. Most nursing
programs have adopted these new approaches and technologies. The ultimate goal is to shift health care decisions, choices, and actions to a higher, more scientific, research and theoretically-based level. One of the strongest and most far-reaching current trends in health care is the application of evidence - based practice through the development of research and information technology/informatics. This trend is visible across all sectors of nursing, including practice, education, research, and administration. The rationale behind this trend is to improve client care by selecting best practice options grounded in viable research, and to expand the theoretical foundations of all health professions. Most nursing
programs have adopted these new approaches and technologies. The ultimate goal is to shift health care decisions, choices, and actions to a higher, more scientific, research and theoretically-based level.
The Advent of Evidence Based Practice
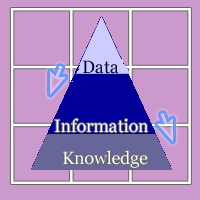 Information technology breakthroughs have been a key factor in the development of evidence based practice (EBP) and has supported this growing trend to promote it in nursing and other health care disciplines such as medicine (Georgiou. 2002; Johnson, 2004; Skiba, 2005). A common conceptual basis for nursing and health informatics consists of a triad of data, information, and knowledge (Graves & Corcoran, 1989; Staggers & Bagley-Thompson, 2001), where nursing data gathered manually, or using computers and other technologies are combined and categorized into meaningful information, which when reflected on and logically analyzed, become nursing knowledge. These elements are arranged in a hierarchy, with data at the base of the model providing the basis for establishing information and leading in turn to the potential generation of knowledge. The informatics model converges closely with the principles, aims and tasks of evidence-based medicine (EBM), particularly as they relate to searching, appraising, reviewing and utilizing information and research (Georgiou, 2002, p. 127). Information technology breakthroughs have been a key factor in the development of evidence based practice (EBP) and has supported this growing trend to promote it in nursing and other health care disciplines such as medicine (Georgiou. 2002; Johnson, 2004; Skiba, 2005). A common conceptual basis for nursing and health informatics consists of a triad of data, information, and knowledge (Graves & Corcoran, 1989; Staggers & Bagley-Thompson, 2001), where nursing data gathered manually, or using computers and other technologies are combined and categorized into meaningful information, which when reflected on and logically analyzed, become nursing knowledge. These elements are arranged in a hierarchy, with data at the base of the model providing the basis for establishing information and leading in turn to the potential generation of knowledge. The informatics model converges closely with the principles, aims and tasks of evidence-based medicine (EBM), particularly as they relate to searching, appraising, reviewing and utilizing information and research (Georgiou, 2002, p. 127).
 This approach to knowledge development, and decision-making within practice is not a new one. The seeds of evidence-based practice were first sown in Newtonian times and further developed through the rise of positivism and scientism. The informatics process traces its origins to the functions of taxonomy and classification as they developed in the 19th century. Early statisticians used and developed classification systems as repositories of knowledge established from data and information. They in turn developed an informatics model consisting of three essential parts arranged hierarchically, with data at the bottom, an intermediary layer of information, and topped by a knowledge layer (Georgiou, 2002, p. 128). This approach to knowledge development, and decision-making within practice is not a new one. The seeds of evidence-based practice were first sown in Newtonian times and further developed through the rise of positivism and scientism. The informatics process traces its origins to the functions of taxonomy and classification as they developed in the 19th century. Early statisticians used and developed classification systems as repositories of knowledge established from data and information. They in turn developed an informatics model consisting of three essential parts arranged hierarchically, with data at the bottom, an intermediary layer of information, and topped by a knowledge layer (Georgiou, 2002, p. 128).
 The use of information technologies has perpetuated this approach to clinical decision making through various applications. The astounding collection of statistics available electronically is one such application. The development of digital nursing languages and nomenclatures are another important supportive application. The ability to use computers for every stage of the research process, both quantitative and qualitative is another key application. Modern health care administration is strongly focused on the incorporation of all three of these developments to shape the activities, mandate, and focus of contemporary nursing. The use of information technologies has perpetuated this approach to clinical decision making through various applications. The astounding collection of statistics available electronically is one such application. The development of digital nursing languages and nomenclatures are another important supportive application. The ability to use computers for every stage of the research process, both quantitative and qualitative is another key application. Modern health care administration is strongly focused on the incorporation of all three of these developments to shape the activities, mandate, and focus of contemporary nursing.
While EBP is promoted as the definitive way to boost nursing's credibility, respectability, and uniqueness,  there is also an almost invisible undercurrent of control and conformity that may threaten the essence of genuine nursing care. There are some who criticize EBM as statistically driven rather than scientifically driven, and complain that the health service has been forcibly unified under a single quality assurance system - easily regulated by politicians, bureaucrats, and their statistical technicians (Georgiou, 2002, p. 129). Still, much of the nursing literature, especially nursing administration literature supports this approach to planning routine care as well as advancing the nursing profession. Data transformed into information and further transformed into knowledge assists healthcare staff in making knowledge-based decisions--choices based on the patient's total healthcare picture. Systemwide data provides a means to analyze overall process effectiveness and to spot areas needing change. This type of information management is instrumental in analyzing indicators that correlate nursing actions--such as the percentage of R.N. care hours versus all nursing care hours--with patient outcomes(Ball, 2005, p. 1). there is also an almost invisible undercurrent of control and conformity that may threaten the essence of genuine nursing care. There are some who criticize EBM as statistically driven rather than scientifically driven, and complain that the health service has been forcibly unified under a single quality assurance system - easily regulated by politicians, bureaucrats, and their statistical technicians (Georgiou, 2002, p. 129). Still, much of the nursing literature, especially nursing administration literature supports this approach to planning routine care as well as advancing the nursing profession. Data transformed into information and further transformed into knowledge assists healthcare staff in making knowledge-based decisions--choices based on the patient's total healthcare picture. Systemwide data provides a means to analyze overall process effectiveness and to spot areas needing change. This type of information management is instrumental in analyzing indicators that correlate nursing actions--such as the percentage of R.N. care hours versus all nursing care hours--with patient outcomes(Ball, 2005, p. 1).
 Information processing has been a vital part of nursing, far longer than the availability of computers and ICTs. Information processing and communication are centrally involved in virtually all health care activities, including obtaining and recording information about patients; communication among health care professionals; accessing medical literature; selecting diagnostic procedures; interpreting laboratory results; and collecting clinical research data (Georgiou, 2002, p. 128). ICT advancement has made it possible to utilize technology to quicken all of these activities, to access a digitally stored pool of literature, statistics, and research data to assist in decisions, and provide a language for nurses to use to record and plan individual client care. Information processing has been a vital part of nursing, far longer than the availability of computers and ICTs. Information processing and communication are centrally involved in virtually all health care activities, including obtaining and recording information about patients; communication among health care professionals; accessing medical literature; selecting diagnostic procedures; interpreting laboratory results; and collecting clinical research data (Georgiou, 2002, p. 128). ICT advancement has made it possible to utilize technology to quicken all of these activities, to access a digitally stored pool of literature, statistics, and research data to assist in decisions, and provide a language for nurses to use to record and plan individual client care.
 This advancement in access to quality data, information and knowledge can be a very valuable resource for practicing nurses, especially if they also have the time and technological support to gather, absorb, reflect on, and synthesize the information that they find within the digital collections. However, the mechanistic daily operations of the health care system leave little time for this knowledge development and application to occur. Today, nurses are responsible for increasingly machine oriented health care dominated by administration and bureaucratic structures (Barnard, 1997, p. 126). In theory, evidenced based practice appears to support quality client care, but in reality, it often becomes a means to further the modernist focus on quality assurance, regulation, standardization, and accreditation: essentially, the workings of the system (Buckeridge, 1999). The generation of knowledge proceeds through a complex process of induction, deduction, and assessment, itself subject to scientific debate and further trials and experimentation. ...Moreover, the whole process cannot be divorced from the social, economic and even political influences that impact upon any decision making exercise (Georgiou, 2002, p. 128). This advancement in access to quality data, information and knowledge can be a very valuable resource for practicing nurses, especially if they also have the time and technological support to gather, absorb, reflect on, and synthesize the information that they find within the digital collections. However, the mechanistic daily operations of the health care system leave little time for this knowledge development and application to occur. Today, nurses are responsible for increasingly machine oriented health care dominated by administration and bureaucratic structures (Barnard, 1997, p. 126). In theory, evidenced based practice appears to support quality client care, but in reality, it often becomes a means to further the modernist focus on quality assurance, regulation, standardization, and accreditation: essentially, the workings of the system (Buckeridge, 1999). The generation of knowledge proceeds through a complex process of induction, deduction, and assessment, itself subject to scientific debate and further trials and experimentation. ...Moreover, the whole process cannot be divorced from the social, economic and even political influences that impact upon any decision making exercise (Georgiou, 2002, p. 128).
Maintaining the Organizational Machine
 Since practicing nurses have little time to actually engage in the process of applying research, statistics, and other data to their practice, the EBP movement is often put into motion under the command of nurse leaders (Nurse Informatics Specialists, Nurse Managers, Clinical Nurse Specialists, Clinicians, and so on) through the discerning application of technology to practice directives. Administrators quantify technology benefits that increase productivity, streamline work processes, or impact patient quality and safety. Technology options such as clinical documentation systems, bar coding, medication administration, computerized provider order entry (CPOE), specialty systems, inventory, charge capture, and workflow management are maturing (Parker, 2004, p. 41) and become the ultimate rationale for applying informatics to nursing practice. Since practicing nurses have little time to actually engage in the process of applying research, statistics, and other data to their practice, the EBP movement is often put into motion under the command of nurse leaders (Nurse Informatics Specialists, Nurse Managers, Clinical Nurse Specialists, Clinicians, and so on) through the discerning application of technology to practice directives. Administrators quantify technology benefits that increase productivity, streamline work processes, or impact patient quality and safety. Technology options such as clinical documentation systems, bar coding, medication administration, computerized provider order entry (CPOE), specialty systems, inventory, charge capture, and workflow management are maturing (Parker, 2004, p. 41) and become the ultimate rationale for applying informatics to nursing practice.
 Likewise, the selection of nursing information systems is often done by administrative nurses, often through the lens of organizational operations rather than the actual needs of the nurses who use them or the clients they serve. Nurse administrators must work directly with the CIO and nurse informatics specialist in developing and deploying systems to convert this data into useful information. The nurse administrator must help develop the IS strategic vision to ensure selection of the hardware and software needed for applications that can be used in many units or linked with other facilities. Likewise, the selection of nursing information systems is often done by administrative nurses, often through the lens of organizational operations rather than the actual needs of the nurses who use them or the clients they serve. Nurse administrators must work directly with the CIO and nurse informatics specialist in developing and deploying systems to convert this data into useful information. The nurse administrator must help develop the IS strategic vision to ensure selection of the hardware and software needed for applications that can be used in many units or linked with other facilities.  These key applications will provide fundamental systems support for nursing department operations, such as workforce, financial and quality management systems. Systems for patient classification (e.g., analyzing patient acuity level to determining level of care needed) are critical to support nursing administration functions. In financial management, linking patient classification data, staffing requirements, and evidence-based practice data to a budget methodology can help justify the nursing department's annual operating budget and expedite budget preparation (Ball, 2005, p. 2). These key applications will provide fundamental systems support for nursing department operations, such as workforce, financial and quality management systems. Systems for patient classification (e.g., analyzing patient acuity level to determining level of care needed) are critical to support nursing administration functions. In financial management, linking patient classification data, staffing requirements, and evidence-based practice data to a budget methodology can help justify the nursing department's annual operating budget and expedite budget preparation (Ball, 2005, p. 2).
 Although the use of technology to support EBP can be a valuable process in providing the best care possible, it is often restricted to a justifying role for the adoption of particular rituals and practices, in the name of technique. The current trends in health care motivate nursing leaders and hospital administration to align strategic objectives with technological adoption with the end goal of remaining financially competitive (Mazzella Ebstein, 2004). Technique refers to the formation of systems comprised of human, organizational, political, and economic structures which are aimed toward the absolute efficiency of methods and means in each field of human endeavor. Technique, not technology has increasingly structured collective behaviour and influenced individual lives, cultures, and professional perspectives. Many aspects of nursing and health care are structured in accordance with technical demands arising from relationships that develop because of technique which emphasize a primacy of means, efficiency, and rational order. Technique does not attend to such phenomena as individual and cultural difference. The purpose of technique is to reproduce itself; it is the center of its own attention (Barnard & Sandelowski, 2001, p. 372). Although the use of technology to support EBP can be a valuable process in providing the best care possible, it is often restricted to a justifying role for the adoption of particular rituals and practices, in the name of technique. The current trends in health care motivate nursing leaders and hospital administration to align strategic objectives with technological adoption with the end goal of remaining financially competitive (Mazzella Ebstein, 2004). Technique refers to the formation of systems comprised of human, organizational, political, and economic structures which are aimed toward the absolute efficiency of methods and means in each field of human endeavor. Technique, not technology has increasingly structured collective behaviour and influenced individual lives, cultures, and professional perspectives. Many aspects of nursing and health care are structured in accordance with technical demands arising from relationships that develop because of technique which emphasize a primacy of means, efficiency, and rational order. Technique does not attend to such phenomena as individual and cultural difference. The purpose of technique is to reproduce itself; it is the center of its own attention (Barnard & Sandelowski, 2001, p. 372).
 The modernist health care system demands that nurses operate within this technique driven environment, and nurses have learned to embrace this way of acting and being while providing client care. We nurses have expressed concern over the impact of technology but have embraced technique. Yet it is technique that has made nursing technological not objects, machines, automata, or equipment (Barnard & Sandelowski, 2001, p. 372). This focus on technique places nurses within a whirlwind of regulations and standardization that threatens their ability to care for clients in a phenomenological, individualized way. Because of technique, there can be over emphasis on the maximization of efficiency, specialization of practice and development of conformity and sameness in product, process, and thought. Accordingly, it is technique, not technological objects per se that we must confront, as we have delegated to technique the power of decision making and have relied on technique for the development of professional status (p. 372). The modernist health care system demands that nurses operate within this technique driven environment, and nurses have learned to embrace this way of acting and being while providing client care. We nurses have expressed concern over the impact of technology but have embraced technique. Yet it is technique that has made nursing technological not objects, machines, automata, or equipment (Barnard & Sandelowski, 2001, p. 372). This focus on technique places nurses within a whirlwind of regulations and standardization that threatens their ability to care for clients in a phenomenological, individualized way. Because of technique, there can be over emphasis on the maximization of efficiency, specialization of practice and development of conformity and sameness in product, process, and thought. Accordingly, it is technique, not technological objects per se that we must confront, as we have delegated to technique the power of decision making and have relied on technique for the development of professional status (p. 372).
The Language of Nursing
 An important part of this technique approach to technologically enhanced nursing care is the development of universal nursing data languages. The most prominent of these is the International Classification of Nursing Practice (ICNP) being developed by the International Council of Nurses (ICN). The purpose of the ICNP is to provide a tool for describing and documenting key elements that represent clinical nursing practice (Canadian Nurses Association, 2001, p. 2). In Canada, work on the Health Information: Nursing Components (HI:NC) represents a national initiative to quantify nursing care for computer data recording and analysis. As well, the CIHI completed the development of a new Canadian Classification Health Interventions (CCI) that is currently being implemented in a number of provinces. The CCI was developed to be consistent with concepts and terminology in the ICNP. The classification contains a comprehensive list of diagnostic, therapeutic, support An important part of this technique approach to technologically enhanced nursing care is the development of universal nursing data languages. The most prominent of these is the International Classification of Nursing Practice (ICNP) being developed by the International Council of Nurses (ICN). The purpose of the ICNP is to provide a tool for describing and documenting key elements that represent clinical nursing practice (Canadian Nurses Association, 2001, p. 2). In Canada, work on the Health Information: Nursing Components (HI:NC) represents a national initiative to quantify nursing care for computer data recording and analysis. As well, the CIHI completed the development of a new Canadian Classification Health Interventions (CCI) that is currently being implemented in a number of provinces. The CCI was developed to be consistent with concepts and terminology in the ICNP. The classification contains a comprehensive list of diagnostic, therapeutic, support  and surgical interventions, allowing for the standardized collection of health interventions, regardless of the service provider or service setting (Canadian Nurses Association, 2001, p. 3). The intent of these languages is to ensure that nursing actions are included in the emerging electronic health records being developed at national and international levels. and surgical interventions, allowing for the standardized collection of health interventions, regardless of the service provider or service setting (Canadian Nurses Association, 2001, p. 3). The intent of these languages is to ensure that nursing actions are included in the emerging electronic health records being developed at national and international levels.  This is an important intent, since all too often, nursing actions become merged with the general health data of organizations, and are rendered indistinguishable as actual nursing behaviors. The danger though is that the unique qualities of nursing: the caring, the empathy, the customization of client care to suit client preferences and genuine needs may get lost or remain unnamed since they do not fit any of the designated data categories. Thus, the recorded data may only reflect the information needed for bureaucratic operations, rather than provide a continuum of individualized care for the client. This is an important intent, since all too often, nursing actions become merged with the general health data of organizations, and are rendered indistinguishable as actual nursing behaviors. The danger though is that the unique qualities of nursing: the caring, the empathy, the customization of client care to suit client preferences and genuine needs may get lost or remain unnamed since they do not fit any of the designated data categories. Thus, the recorded data may only reflect the information needed for bureaucratic operations, rather than provide a continuum of individualized care for the client.
It is important then, for nurses to become critically aware of how and why they are using computers in nursing care, and that they become knowledgeable and skilled enough to influence the way nursing care becomes digitized. The nation is at a tipping point in applying enabling technologies to healthcare. With the push coming from the federal government and all corners of the field, this is indeed a far-reaching revolution.  The time has come for healthcare to leave the manual tools of the past in the past and turn to the enablers of the 21st century. The nursing profession is being transformed to meet the needs of the new world and will be a major player in the revolution (Ball, 2005, p. 2). It is up to nurses as a group to choose whether they will be major players who simply perpetuate the modernistic workings of the system, or learn to apply technology to support the provision of true client-centered and supportive care. Technology demands levels of attention, time and commitment that can be arduous for a nurse and inappropriate to the needs of patients and the clinical environment (Barnard, 2000, p. 1138). The time has come for healthcare to leave the manual tools of the past in the past and turn to the enablers of the 21st century. The nursing profession is being transformed to meet the needs of the new world and will be a major player in the revolution (Ball, 2005, p. 2). It is up to nurses as a group to choose whether they will be major players who simply perpetuate the modernistic workings of the system, or learn to apply technology to support the provision of true client-centered and supportive care. Technology demands levels of attention, time and commitment that can be arduous for a nurse and inappropriate to the needs of patients and the clinical environment (Barnard, 2000, p. 1138).
The literature supports the notion that nurses often choose to resist the assimilation of information technology into nursing care on the grounds that it interferes with their ability to provide genuine, client-centered nursing care. Nurses are among many groups who still adhere to a humanist view of technology on the nonhuman and nonnatural side of the human/nonhuman, nature/artifice divide. We still depict ourselves as the bridge spanning the divide between technology and humane health care. We have already claimed professional ownership of the space between technology and patient, and the responsibility for maintaining humane care in technological environments. Dwelling in this space, we see ourselves as the mediators between two seemingly irreconcilable and disparate forces (Barnard & Sandelowski, 2001, p. 372).
Shifting the System
 For EBP to realistically manifest in nursing practice, a major shift in health care organization and focus must occur. Practicing nurses often lack the knowledge and skill to access the literature and other digital research findings to apply these to practice. As aforementioned, time, rituals and routine expectations are other factors that prevent the proper engagement necessary to genuinely apply EBP to routine nursing care. A study by Tanner and colleagues examined nurses' readiness for evidenced-basedimg For EBP to realistically manifest in nursing practice, a major shift in health care organization and focus must occur. Practicing nurses often lack the knowledge and skill to access the literature and other digital research findings to apply these to practice. As aforementioned, time, rituals and routine expectations are other factors that prevent the proper engagement necessary to genuinely apply EBP to routine nursing care. A study by Tanner and colleagues examined nurses' readiness for evidenced-basedimg  practice, specifically, their information literacy knowledge and competency and their access to research information. The results showed a need in many respondents to: practice, specifically, their information literacy knowledge and competency and their access to research information. The results showed a need in many respondents to:
- acknowledge awareness of a need for information
- identify and retrieve information
- evaluate information for relevance
- integrate information into practice
- and evaluate the effect of the information on the problem or issue (Skiba, 2005, p. 310).
 One key way that these skills are being fostered in future nurses is through the degree preparation afforded by baccalaureates as entry to practice and through the inclusion of nursing informatics in nursing education. As we redesign nursing curricula or develop courses for an evidence-based practice (EBP) world, it is important to consider the essential role of informatics. Recent work by colleagues affirms that an informatics infrastructure is an essential ingredient to EBP and patient safety (Skiba, 2005a, p. 310) where student nurses learn ...critical thinking ICT skills [in how] to define, access, manage, integrate, evaluate, create, and communicate (p. 310). One key way that these skills are being fostered in future nurses is through the degree preparation afforded by baccalaureates as entry to practice and through the inclusion of nursing informatics in nursing education. As we redesign nursing curricula or develop courses for an evidence-based practice (EBP) world, it is important to consider the essential role of informatics. Recent work by colleagues affirms that an informatics infrastructure is an essential ingredient to EBP and patient safety (Skiba, 2005a, p. 310) where student nurses learn ...critical thinking ICT skills [in how] to define, access, manage, integrate, evaluate, create, and communicate (p. 310).
 If nurses develop the skills and abilities to access information, research, and knowledge effortlessly, as well as the time and expectation to carefully plan individualized care using the knowledge they have accessed, the true promise of EBP and nursing informatics could be more clearly realized (Johnson & Ventura 2004). Rather than serving as mere modes of modernist operational management, EBP and informatics could genuinely support nurses in providing expert yet empathetic and individualized care. The Institute of Medicine's report Crossing the Quality Chasm defined 10 characteristics for redesigning health care systems in the 21st century. These characteristics included, among others, the focus on patient-centered care, patient safety as a system property, If nurses develop the skills and abilities to access information, research, and knowledge effortlessly, as well as the time and expectation to carefully plan individualized care using the knowledge they have accessed, the true promise of EBP and nursing informatics could be more clearly realized (Johnson & Ventura 2004). Rather than serving as mere modes of modernist operational management, EBP and informatics could genuinely support nurses in providing expert yet empathetic and individualized care. The Institute of Medicine's report Crossing the Quality Chasm defined 10 characteristics for redesigning health care systems in the 21st century. These characteristics included, among others, the focus on patient-centered care, patient safety as a system property,  free flow of information as a source of knowledge, and decision making that is evidence-based. Evaluating quality and patient safety currently assumes the need to leverage information technology as a tool to achieve a redesigned health care system. Evidence-based practice and using informatics were identified as core competencies for health care professionals in this decade to support the principles of the Quality Chasm report (Johnson, 2004, p. 14). free flow of information as a source of knowledge, and decision making that is evidence-based. Evaluating quality and patient safety currently assumes the need to leverage information technology as a tool to achieve a redesigned health care system. Evidence-based practice and using informatics were identified as core competencies for health care professionals in this decade to support the principles of the Quality Chasm report (Johnson, 2004, p. 14).
 There is an emphasis on just such an approach in nursing education, but in practice, the solution appears to lie in the development of more intelligent and responsive technologies. Expert decision support systems, voice and touch activated computer peripherals, and other user-friendly improvisations are often the focus of new technology developments in health care. Multimodal applications that allow users to interact with computers based on There is an emphasis on just such an approach in nursing education, but in practice, the solution appears to lie in the development of more intelligent and responsive technologies. Expert decision support systems, voice and touch activated computer peripherals, and other user-friendly improvisations are often the focus of new technology developments in health care. Multimodal applications that allow users to interact with computers based on  voice, touch screen, pen, mouse, or keyboard improve user acceptance. Maturing health care technology and continued product enhancements lead to successful application implementation (Parker, 2004, p. 41). A new, exciting, yet frightening branch of research relates to the development of agent technology, where computer programs are being developed to act as personal assistants to human users. This wave of technological research and development embraces another perspective of informatics where technology is regarded as an agent, a responsive phenomena that can interact and engage with humans as unique entities with innate agency. voice, touch screen, pen, mouse, or keyboard improve user acceptance. Maturing health care technology and continued product enhancements lead to successful application implementation (Parker, 2004, p. 41). A new, exciting, yet frightening branch of research relates to the development of agent technology, where computer programs are being developed to act as personal assistants to human users. This wave of technological research and development embraces another perspective of informatics where technology is regarded as an agent, a responsive phenomena that can interact and engage with humans as unique entities with innate agency.
|

|
